Table of Contents >> Show >> Hide
- A Medical Delay That Became a Public Wake-Up Call
- Who Is Amanda Harris, and What Happened?
- Why Brain Tumor Surgery Can Depend on ICU Capacity
- The Unvaccinated Hospitalization Problem
- How COVID Surges Delayed Surgeries Across the United States
- The Emotional Cost of Waiting for Brain Surgery
- Why Blame Alone Does Not Solve the Problem
- What This Story Teaches About Public Health
- Practical Lessons for Patients Facing Delayed Surgery
- Related Experiences: Living in the Waiting Room of Uncertainty
- Conclusion: Amanda’s Story Is About More Than One Surgery
Note: This article is written for informational and editorial purposes only. It is not medical advice. Anyone dealing with a brain tumor, postponed surgery, COVID-19 concerns, or vaccination questions should speak directly with licensed medical professionals.
A Medical Delay That Became a Public Wake-Up Call
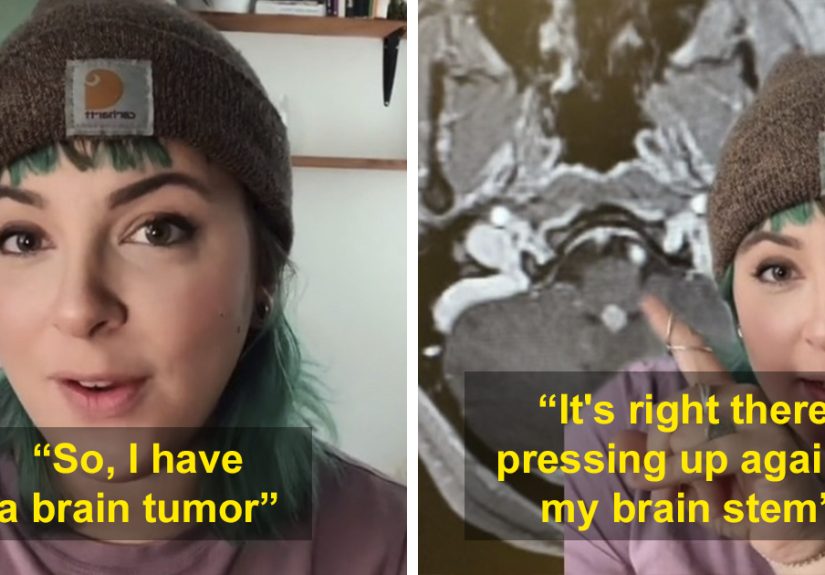
Few sentences are heavier than “you have a brain tumor.” Now imagine hearing the next sentence: “We cannot remove it yet because there are no ICU beds available.” That was the terrifying reality shared publicly by Amanda Harris, a Portland artist and woodworker whose brain tumor surgery was delayed during a COVID-19 hospital surge. Her story spread because it put a human face on something many people discussed only in charts, dashboards, and tense dinner-table arguments: when hospitals are full, the consequences do not stop with COVID patients.
Amanda’s situation was especially frightening because the tumor had not yet been fully classified as benign or malignant. In many brain tumor cases, doctors may not know exactly what type of tumor they are dealing with until tissue is removed or sampled. That means surgery is not just treatment; it can also be the key to diagnosis, staging, planning, and peace of mind. Waiting is not like waiting for a haircut appointment. It is more like living with a fire alarm ringing inside your skull while someone tells you the fire department is busy.
The story became controversial because Amanda connected her delayed surgery to the pressure unvaccinated COVID-19 patients were placing on hospitals. Her frustration was not just personal anger. It reflected a broader public-health reality during the Delta and Omicron waves: unvaccinated people were far more likely to need hospitalization, and hospitals across the United States repeatedly delayed surgeries to preserve beds, staff, ventilators, and intensive-care capacity. The result was a cruel domino effect. One person’s preventable severe illness could indirectly delay another person’s cancer operation, heart procedure, transplant evaluation, or neurological surgery.
Who Is Amanda Harris, and What Happened?
Amanda Harris, known online as an artist and maker, shared her experience on TikTok after learning that her brain tumor surgery could not move forward as expected. According to public reporting, she had been waiting for a surgery date after months of imaging, medical appointments, and uncertainty. The tumor was described as potentially serious, and its exact nature could not be confirmed until after resection. That uncertainty alone would be enough to flatten most people emotionally. Add a hospital capacity crisis, and the situation becomes almost absurd in the worst possible way.
In her videos and interview comments, Amanda explained that her doctors needed an ICU bed available after surgery. That requirement makes sense. Brain tumor surgery can involve swelling, bleeding risk, neurological monitoring, airway management, seizures, blood pressure control, and other complications that require immediate expert attention. An ICU bed is not a luxury upgrade, like extra legroom on a flight. It is part of the safety plan.
Her message was direct: when intensive care beds are occupied by patients with severe COVID-19, other patients can be pushed into limbo. Amanda pleaded with people to get vaccinated and boosted, not only to protect themselves but also to protect the healthcare system that everyone depends on. Her fear was not theoretical. She was not arguing about politics from a couch. She was waiting for brain surgery and crying into the camera because she did not know when she would get the care she needed.
Why Brain Tumor Surgery Can Depend on ICU Capacity
Brain tumor surgery is not one single procedure. Depending on tumor type, location, size, symptoms, and overall health, treatment may involve craniotomy, biopsy, stereotactic radiosurgery, laser ablation, radiation, chemotherapy, targeted therapy, surveillance, or a combination of approaches. But when surgeons decide that a tumor needs to be removed or sampled, timing can matter. Some tumors grow slowly. Others behave aggressively. Some press on critical structures, causing headaches, seizures, vision changes, weakness, dizziness, or cognitive problems. In other words, the brain is not exactly a roomy studio apartment with spare corners for unwanted guests.
For many patients, the operation itself is only one part of the medical plan. The hours after surgery can be just as important. Doctors may need to watch for swelling, bleeding, changes in speech or movement, altered consciousness, seizures, or breathing problems. That is why ICU access can be essential even if the surgery is scheduled and the surgical team is ready. Without a safe place for recovery, the operation may be postponed.
This is where public health becomes personal. Hospital resources are shared resources. A community does not have separate hospitals for “COVID problems” and “everyone else problems.” There is one pool of nurses, respiratory therapists, surgeons, anesthesiologists, beds, operating rooms, and ICU capacity. When that pool is overwhelmed, patients who never tested positive for COVID-19 can still suffer because of COVID-19.
The Unvaccinated Hospitalization Problem
During major pandemic waves, public-health data consistently showed that vaccinated people were much less likely to suffer severe COVID-19 outcomes than unvaccinated people. Vaccines were never a magic force field that guaranteed no infection. That misunderstanding caused endless confusion. Their biggest value was reducing the risk of severe illness, hospitalization, ICU admission, and death. In plain English: the vaccine’s job was not always to stop the virus at the front door; often, it was to stop the virus from burning down the whole house.
That difference mattered enormously for hospitals. When large numbers of unvaccinated people became severely ill at the same time, emergency rooms filled up, ICUs reached capacity, and nurses were stretched beyond safe limits. Some hospitals transferred patients hundreds of miles. Others postponed non-emergency surgeries. “Elective surgery” became one of the most misunderstood phrases of the pandemic. It did not always mean optional or cosmetic. It often meant scheduled, necessary, and sometimes life-changing, but not immediately required within the next few hours.
That distinction is painfully important. A brain tumor removal may be scheduled rather than performed in the emergency room, but that does not make it emotionally light or medically trivial. A delayed operation can mean prolonged pain, worsening symptoms, increased anxiety, lost income, more scans, more appointments, and the horrible psychological burden of not knowing what is growing inside your body.
How COVID Surges Delayed Surgeries Across the United States
Amanda’s story was not an isolated oddity. Hospitals across the United States delayed surgeries during COVID surges to preserve beds and staff. In some regions, the problem was not simply physical beds. It was staffed beds. A bed without trained nurses is furniture. A ventilator without respiratory therapists is equipment in a corner. Modern medicine depends on people, and by late 2021 and early 2022, many healthcare workers were exhausted, sick, traumatized, burned out, or leaving the profession.
National analyses found that pandemic pressure reduced surgical volume and disrupted care well beyond the earliest lockdown period. Cancer care was altered, routine procedures were deferred, and backlogs grew. Even after vaccines became available, new variants and uneven vaccination rates continued to strain the system. For patients, the result was a waiting game no one wanted to play.
In theory, hospitals triage patients to protect those at greatest immediate risk. In practice, triage is emotionally brutal. Doctors and administrators must decide which procedures can safely wait and which cannot. Those decisions are guided by medical urgency, available resources, staffing, ICU capacity, and risk of harm from delay. Nobody becomes a surgeon because they dream of canceling surgery. Nobody becomes a nurse because they want to explain to a frightened patient that there is no room. Yet during COVID surges, healthcare teams had to deliver exactly those conversations again and again.
The Emotional Cost of Waiting for Brain Surgery
The medical facts are alarming, but the emotional reality is even harder to capture. Waiting for brain tumor surgery can feel like being trapped in a hallway between two locked doors. Behind one door is treatment. Behind the other is diagnosis. You cannot move forward until someone gives you a date, a bed, and a plan.
Patients often describe this period as surreal. One minute they are answering work emails, folding laundry, or buying groceries. The next, they are memorizing medical terminology they never wanted to learn: resection, craniotomy, biopsy, edema, malignancy, neurosurgery, ICU. Their calendar changes from birthdays and deadlines to MRI appointments and insurance calls. Friends may say, “Stay positive,” which is kind, but not always useful. Positivity does not remove a tumor, and it certainly does not create an ICU bed.
Amanda’s public grief resonated because she expressed what many patients are trained to hide. She was scared. She was heartbroken. She was angry. And frankly, those feelings made sense. When your health depends on a system under strain, you are not just fighting illness. You are fighting logistics, uncertainty, and the feeling that your life has become a number in a queue.
Why Blame Alone Does Not Solve the Problem
It is easy to turn stories like Amanda’s into a shouting match: vaccinated versus unvaccinated, personal freedom versus public responsibility, individual choice versus collective consequence. But a more useful conversation starts with a difficult truth: choices in a pandemic do not remain private when they affect hospital capacity.
That does not mean every unvaccinated person had the same reason for remaining unvaccinated. Some people were misled by misinformation. Some were afraid. Some had access issues. Some distrusted institutions because of past harm. Some were medically advised to delay or avoid vaccination. And yes, some simply refused. A humane public-health response should be honest enough to recognize those differences while still stating the evidence clearly: widespread vaccination reduces severe disease and helps protect hospital systems.
The goal should not be to dehumanize unvaccinated patients. Doctors treat people because they are sick, not because they made perfect choices. But compassion for hospitalized COVID patients can coexist with compassion for patients whose surgeries were delayed. Amanda’s story is not about deciding who deserves care. It is about preventing avoidable pressure so fewer people are forced into that terrible competition in the first place.
What This Story Teaches About Public Health
Public health is often invisible when it works. Nobody throws a parade for the ICU bed that stayed open, the outbreak that never happened, or the surgery that went ahead on schedule because community transmission stayed low. But when public health fails, the effects become painfully visible. Ambulances wait. Nurses cry in break rooms. Families beg for transfers. Patients like Amanda wait for operations that should already be on the calendar.
The lesson is not only about COVID-19 vaccines. It is about how connected healthcare really is. Flu shots, childhood vaccines, masking when sick, staying home during contagious illness, improving indoor air quality, supporting hospitals, funding public-health communication, and reducing medical misinformation all matter because they reduce strain. The healthcare system is not an infinite vending machine where everyone presses a button and receives care instantly. It is a living network, and networks can buckle.
Amanda’s story also shows why patient advocacy matters. She spoke publicly, explained her situation, and urged others to understand the ripple effects of their decisions. Not every patient wants to share personal medical information online, and nobody should feel obligated to do so. But her willingness to speak made an abstract crisis concrete. Sometimes one trembling voice can explain what a thousand statistics cannot.
Practical Lessons for Patients Facing Delayed Surgery
Patients waiting for urgent or semi-urgent surgery should not have to become professional project managers, but many end up doing exactly that. When surgery is delayed, it can help to ask the care team specific questions: What symptoms should trigger an emergency visit? Is the surgery delayed because of ICU capacity, operating-room capacity, staffing, insurance, or medical risk? Are there alternate hospitals in the network? Can the surgeon place the patient on a cancellation list? Is there a nurse navigator or social worker who can help coordinate updates?
Patients can also keep a written symptom log. New headaches, seizures, weakness, vision changes, confusion, nausea, balance problems, or speech changes should be reported promptly. For brain tumor patients, even subtle changes can matter. A log helps doctors see patterns and may support reassessment of urgency.
Family and friends can help by doing practical things instead of offering vague encouragement. Drive the patient to appointments. Take notes during calls. Cook meals. Help organize medical documents. Sit quietly without trying to fix the unfixable. Send one text that says, “No need to reply; I’m thinking of you,” and congratulations, you have already outperformed half the internet.
Related Experiences: Living in the Waiting Room of Uncertainty
People who have waited for major surgery during a hospital surge often describe the experience as a strange mix of fear, boredom, guilt, and helplessness. The fear is obvious. You worry that your condition will worsen while you wait. You worry that a scan will show growth. You worry that your doctor will call with bad news, or worse, no news at all. But the boredom is real too. Life becomes a loop of checking your phone, refreshing patient portals, rereading discharge instructions, and trying not to search symptoms online at 2 a.m. The internet, as everyone knows, can turn a mild headache into a Victorian death scene in under six clicks.
One common experience is feeling suspended between identities. You are not fully a patient in treatment yet, but you are not living your old life either. You may look fine to strangers. You may even sound fine on the phone. Inside, though, every plan comes with an asterisk. Can you commit to a work project? Maybe. Can you travel? Probably not. Can you make holiday plans? Only if everyone is comfortable with the phrase “subject to sudden neurosurgery.”
Another experience is anger that has nowhere clean to go. Patients may be angry at the virus, angry at the hospital, angry at politicians, angry at misinformation, angry at people who refused vaccination, angry at their own bodies, and then guilty for being angry because healthcare workers are clearly doing their best. That emotional traffic jam is exhausting. It helps to name it: anger during medical uncertainty is not a personality flaw. It is a normal response to feeling unsafe and powerless.
Caregivers live through their own version of this uncertainty. They may become the person who answers calls, tracks medications, researches hospitals, updates relatives, and tries to stay calm while quietly falling apart in the shower. They are expected to be strong, but strength is not the same as numbness. Caregivers need rest, food, support, and permission to admit that they are scared too.
Healthcare workers also carry these stories. A nurse who tells a patient that surgery is delayed because no ICU bed is available is not reading from a customer-service script. They know there is a person behind the chart. They know delay can mean suffering. Many clinicians spent the pandemic absorbing anger from every direction while trying to keep patients alive with too few hands and too many alarms.
The most painful part of these experiences is that they reveal how fragile “normal” can be. Before illness, a hospital may feel like a place that simply exists in the background. After diagnosis, it becomes the center of the universe. When that center is overwhelmed, patients learn a hard truth: healthcare access is not only about having a doctor. It is about having space, staff, equipment, community cooperation, and systems that can bend without breaking.
And yet, many patients also discover a stubborn kind of resilience. They learn to ask better questions. They learn which friends show up. They learn that crying in a parking lot does not mean they are failing. They learn that humor can sit beside fear without disrespecting it. A joke will not remove a tumor, but sometimes it can help a person breathe for ten more seconds. On the worst days, ten seconds counts.
Conclusion: Amanda’s Story Is About More Than One Surgery
The story of a woman with a brain tumor scared and heartbroken because she could not get it removed is not just a viral headline. It is a snapshot of how individual medical choices, hospital capacity, misinformation, pandemic fatigue, and public responsibility collided in real life. Amanda Harris became part of a larger conversation because her situation exposed the hidden cost of overwhelmed hospitals: the patients waiting offstage.
Her story should not be remembered only as an argument about vaccination. It should be remembered as a reminder that healthcare is shared infrastructure. When fewer people become severely ill from preventable disease, more beds remain available for brain tumors, strokes, heart attacks, car crashes, complicated births, cancer surgeries, and emergencies no one sees coming. Public health is not abstract. Sometimes it is the ICU bed that lets a surgeon say, “We can operate tomorrow.”





