Table of Contents >> Show >> Hide
- What Is Femoral Neuropathy?
- Common Symptoms of Femoral Neuropathy
- Femoral Neuropathy Causes
- How Doctors Diagnose Femoral Neuropathy
- Conditions That Can Mimic Femoral Neuropathy
- Femoral Neuropathy Treatment
- Recovery Outlook: How Long Does Femoral Neuropathy Last?
- Femoral Neuropathy Exercises
- Lifestyle Tips That Support Nerve Recovery
- When to See a Doctor
- Experience-Based Section: What Living With Femoral Neuropathy Can Feel Like
- Conclusion
- SEO Tags
Femoral neuropathy is what happens when the femoral nervethe large nerve that helps power the front of the thighgets irritated, compressed, stretched, inflamed, or injured. The result can feel like your leg suddenly forgot the group project: thigh pain, numbness, tingling, knee weakness, trouble climbing stairs, or a knee that buckles at the worst possible moment.
The good news is that many cases improve with the right diagnosis, smart treatment, and a careful rehabilitation plan. The less-good news is that femoral neuropathy can come from several different causes, so guessing is not a great strategy. A sore thigh after sitting awkwardly may be simple. New weakness, severe pain, or loss of function deserves medical attention.
What Is Femoral Neuropathy?
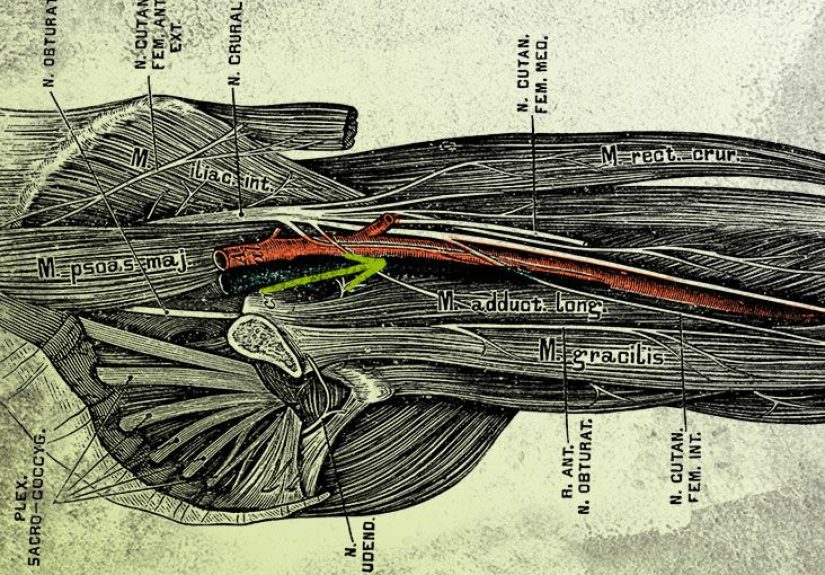
Femoral neuropathy, also called femoral nerve dysfunction or femoral mononeuropathy, is damage or impaired function of the femoral nerve. This nerve starts from the lumbar spine nerve roots, mainly L2 to L4, travels through the pelvis, passes near the groin, and continues into the front of the thigh.
The femoral nerve has two major jobs. First, it helps control muscles that flex the hip and straighten the knee, especially the quadriceps. Second, it carries sensation from parts of the front and inner thigh and, through the saphenous nerve branch, the inner lower leg and foot. When this nerve is not working well, both movement and sensation may be affected.
That is why femoral neuropathy is more than “just leg pain.” It can interfere with walking, standing from a chair, climbing stairs, getting out of a car, exercising, and even feeling confident on uneven ground. The condition can be mild and temporary, or it can be more serious if the nerve is severely compressed or injured.
Common Symptoms of Femoral Neuropathy
Symptoms depend on where the nerve is affected and how severe the injury is. Some people notice mostly sensory symptoms, while others mainly experience weakness. Many have both.
Typical symptoms include:
- Pain in the front of the thigh, groin, hip, or inner leg
- Numbness, tingling, burning, or “pins and needles” in the thigh
- Weakness when straightening the knee
- Difficulty climbing stairs, especially going down
- A knee that buckles or feels unstable
- Reduced or absent knee reflex
- Muscle shrinking in the quadriceps if weakness lasts a long time
- Problems standing up from a low chair
- Changes in walking pattern, such as limping or locking the knee
A practical example: someone with femoral neuropathy may be able to walk on flat ground but feel betrayed by stairs. Going upstairs requires hip and thigh strength; going downstairs demands controlled knee extension. When the quadriceps are weak, the knee may wobble like a folding lawn chair in a windstorm.
Femoral Neuropathy Causes
Femoral neuropathy is not a single-cause condition. The femoral nerve can be affected by pressure, trauma, surgery, metabolic disease, inflammation, bleeding, tumors, or prolonged positioning. Finding the cause matters because treatment should target the reason the nerve is struggling.
1. Direct injury or trauma
A fall, pelvic fracture, hip injury, sports trauma, or deep wound near the groin or thigh can damage the femoral nerve. Trauma may stretch, bruise, compress, or cut nerve fibers. In some cases, the injury is obvious. In others, symptoms appear gradually after swelling or scar tissue develops.
2. Compression from prolonged pressure
Pressure on the nerve can happen from long periods in certain positions, especially if the hip is held in extreme flexion, abduction, or rotation. Surgical positioning, prolonged bed rest, tight belts, braces, casts, or certain occupational postures may contribute. The femoral nerve is not dramatic; it simply dislikes being squeezed for too long.
3. Surgery-related femoral nerve injury
Femoral neuropathy may occur after pelvic, abdominal, gynecologic, urologic, vascular, or hip surgery. Retractors, swelling, surgical positioning, local trauma, or reduced blood supply can affect the nerve. It is considered uncommon, but when it happens, it can be frustrating because the person may wake up from surgery with unexpected thigh weakness or numbness.
4. Diabetes and proximal neuropathy
People with diabetes can develop different types of nerve damage. One related condition is diabetic proximal neuropathy, also known as diabetic amyotrophy or diabetic lumbosacral radiculoplexus neuropathy. It often causes sudden or progressive pain in the hip, buttock, or thigh, followed by weakness and muscle loss. It may affect one side first and can improve slowly over months or years.
5. Bleeding or hematoma near the nerve
A retroperitoneal hematomableeding deep in the back of the abdomencan compress the femoral nerve. This is more likely in people taking blood thinners, people with bleeding disorders, or after trauma or procedures. This cause can be serious and needs prompt medical evaluation, especially if severe groin or thigh pain appears with weakness.
6. Tumors, cysts, or masses
A mass in the pelvis, abdomen, hip region, or groin can press on the femoral nerve. This is less common than mechanical irritation or diabetes-related nerve disease, but it is one reason imaging may be ordered when symptoms are unexplained, progressive, or associated with other concerning signs.
7. Inflammation, infection, or autoimmune disease
Inflammatory neuropathies and certain autoimmune conditions may affect peripheral nerves, including branches in the lumbar plexus. Infections or inflammatory reactions can also irritate nerves. These causes usually require a broader medical workup rather than a simple “stretch it and hope” plan.
8. Idiopathic cases
Sometimes no clear cause is found. Doctors may call this idiopathic femoral neuropathy. That does not mean the symptoms are imaginary; it means the current testing did not reveal a definite trigger.
How Doctors Diagnose Femoral Neuropathy
Diagnosis begins with a careful history and physical exam. A clinician will ask when symptoms started, whether there was trauma, surgery, diabetes, weight loss, back pain, medication use, blood thinner use, or recent prolonged positioning. Then they will test strength, reflexes, sensation, walking, and hip and knee movement.
Physical examination
During the exam, the doctor may check whether you can straighten your knee against resistance, lift your thigh, feel light touch or pinprick in specific areas, and maintain balance. A reduced knee jerk reflex can point toward femoral nerve or L2-L4 nerve root involvement.
Electromyography and nerve conduction studies
EMG and nerve conduction studies are commonly used to evaluate peripheral nerve problems. Nerve conduction testing measures how well electrical signals travel through the nerve. EMG looks at the electrical activity of muscles. Together, they can help confirm nerve injury, estimate severity, identify whether the problem is mainly nerve fiber loss or conduction block, and distinguish femoral neuropathy from similar conditions.
Imaging tests
MRI, CT, or ultrasound may be used when doctors suspect compression, bleeding, a mass, a pelvic problem, or spine-related causes. Imaging is especially important when symptoms are sudden, severe, progressive, or linked with surgery or trauma.
Blood tests
Blood work may check for diabetes, vitamin deficiencies, inflammation, autoimmune markers, kidney function, thyroid problems, infection, or other metabolic conditions. The exact tests depend on the person’s symptoms and health history.
Conditions That Can Mimic Femoral Neuropathy
Femoral neuropathy can look similar to several other conditions. That is why diagnosis matters. Similar problems include lumbar radiculopathy, hip arthritis, iliopsoas injury, quadriceps tendon injury, meralgia paresthetica, stroke, spinal stenosis, and generalized peripheral neuropathy.
For example, lumbar radiculopathy from a pinched nerve in the lower spine may cause thigh pain and weakness, but the source is the spine rather than the femoral nerve itself. Meralgia paresthetica causes burning or numbness on the outer thigh, but it affects the lateral femoral cutaneous nerve, not the femoral nerve. Same neighborhood, different troublemaker.
Femoral Neuropathy Treatment
Treatment depends on the cause, severity, and how much strength or sensation has been affected. Mild compression may improve with activity modification and physical therapy. Severe compression, bleeding, tumor-related pressure, or major traumatic injury may require urgent or specialized care.
1. Treat the underlying cause
The most important step is addressing the reason the nerve is irritated. That may mean improving blood sugar control in diabetes, adjusting pressure-causing positions, treating inflammation, managing a hematoma, removing a compressive mass, or modifying medications under medical supervision. A nerve cannot fully recover if the same problem keeps poking it with a metaphorical stick.
2. Pain management
Pain relief may include over-the-counter pain relievers, prescription medications for nerve pain, topical treatments, or targeted injections in selected cases. Neuropathic pain often feels burning, electric, or hypersensitive, so regular pain relievers may not always be enough. Doctors may consider medications commonly used for nerve pain depending on the person’s age, health, and other medications.
3. Physical therapy
Physical therapy is often central to recovery. A physical therapist may work on gentle mobility, strengthening, balance, gait training, safe stair practice, and ways to prevent falls. Therapy should be customized because too much exercise too soon can aggravate symptoms, while too little movement can lead to stiffness and weakness.
4. Bracing or assistive devices
If the knee buckles, a brace, cane, walker, or temporary assistive device may help prevent falls. This is not “giving up.” It is engineering. If a bridge is under repair, you add support until it is safe again.
5. Surgery
Surgery is not needed for most cases, but it may be considered if there is severe nerve entrapment, a compressive mass, certain traumatic injuries, or symptoms that do not improve with conservative treatment. The decision depends on imaging, electrodiagnostic findings, symptom severity, and the expected benefit.
Recovery Outlook: How Long Does Femoral Neuropathy Last?
Recovery varies widely. A mild compression injury may improve over weeks to a few months. More significant nerve injury can take many months. Nerves heal slowly, and muscle strength may return gradually. If the nerve has severe damage or the underlying cause remains active, some symptoms may persist.
Better outcomes are more likely when the cause is identified early, compression is relieved, blood sugar is managed when diabetes is involved, and rehabilitation is consistent. Warning signs such as sudden weakness, rapidly worsening pain, loss of bladder or bowel control, fever, unexplained weight loss, or symptoms after trauma or surgery should be checked urgently.
Femoral Neuropathy Exercises
Exercises for femoral neuropathy should be gentle, progressive, and approved by a healthcare professional. The goal is to restore strength, improve flexibility, protect the knee, reduce stiffness, and rebuild confidence with movement. Stop any exercise that causes sharp pain, worsening numbness, or increased weakness.
Safety first
Before exercising, consider these basic rules:
- Use support, such as a chair or wall, if balance is uncertain.
- Avoid aggressive stretching that pulls hard through the groin or front thigh.
- Do not force the knee if it buckles or feels unstable.
- Start with low repetitions and increase slowly.
- Ask a physical therapist about nerve glides before trying them alone.
1. Quad sets
Lie on your back or sit with the leg straight. Tighten the thigh muscle by gently pressing the back of the knee toward the floor or bed. Hold for 3 to 5 seconds, then relax. This helps wake up the quadriceps without requiring much movement.
2. Heel slides
Lie on your back with legs straight. Slowly slide one heel toward your buttocks, bending the knee as far as comfortable. Slide it back out. This encourages hip and knee mobility without heavy loading.
3. Seated knee extension
Sit in a stable chair. Slowly straighten one knee until the lower leg is almost level with the floor. Hold briefly, then lower with control. If this is too hard, reduce the range of motion. If it is easy and approved by your therapist, light ankle weights may be added later.
4. Straight leg raise
Lie on your back with one knee bent and the affected leg straight. Tighten the thigh, then slowly lift the straight leg a short distance. Lower it carefully. This can be challenging for femoral neuropathy, so it should be done only if you can keep the knee straight and avoid pain.
5. Hip abduction
Lie on your side with the affected leg on top. Keep the knee straight but not locked, then slowly lift the top leg slightly and lower it. This strengthens hip muscles that support walking and balance.
6. Gentle hip flexor stretch
A tight hip flexor may increase discomfort in some people. A gentle kneeling or standing hip flexor stretch may help, but it should never feel sharp or electric. Keep the stretch mild and avoid forcing the front of the thigh.
7. Balance practice
Stand near a counter or sturdy chair. Practice shifting weight from one foot to the other. Later, a therapist may add single-leg balance, step-ups, or controlled stair drills. Balance work is especially useful when knee buckling has made walking feel risky.
Lifestyle Tips That Support Nerve Recovery
While lifestyle changes do not magically repair a nerve overnight, they can create better conditions for healing. Think of it as giving the nerve a cleaner desk, better lighting, and fewer annoying emails.
Manage blood sugar
For people with diabetes, blood sugar management is a major part of reducing nerve stress. Consistent medical follow-up, nutrition planning, medication adherence, and regular movement can support nerve health.
Stay active within safe limits
Gentle walking, pool exercise, stationary cycling, or supervised strengthening may help preserve muscle and circulation. The key is pacing. More is not always better. Better is better.
Prevent falls
If the knee buckles, clear tripping hazards, use railings, wear supportive shoes, and consider temporary assistive devices. Falling because you refused a cane is not heroic; it is just adding a sequel nobody asked for.
Avoid prolonged pressure
Change positions regularly, avoid tight compression around the groin, and discuss surgical positioning concerns with your medical team if you have a history of neuropathy.
When to See a Doctor
See a healthcare professional if you have persistent thigh numbness, burning pain, weakness, difficulty walking, or a knee that gives way. Seek urgent care if symptoms come on suddenly, follow trauma or surgery, occur with severe groin or abdominal pain, or are accompanied by fever, major swelling, loss of bladder or bowel control, or rapidly worsening weakness.
Femoral neuropathy is easier to manage when the cause is found early. Waiting months while your leg “acts weird” is not a treatment plan. It is a suspense novel, and your nervous system did not sign a book deal.
Experience-Based Section: What Living With Femoral Neuropathy Can Feel Like
People dealing with femoral neuropathy often describe the experience as confusing before it becomes clear. At first, symptoms may not seem connected. A person may notice an odd burning feeling in the front of the thigh after sitting for a long time. Then stairs become strangely difficult. The knee may buckle once, and suddenly every staircase looks like it was designed by a villain with architectural training.
One common experience is the difference between pain and weakness. Many people expect nerve problems to hurt constantly, but femoral neuropathy can be sneaky. The pain may come and go, while weakness shows up during specific tasks. Getting out of a low chair, stepping into a bathtub, climbing into a car, or walking downhill may reveal the problem more than ordinary walking. That is because the quadriceps must control the knee during those movements. When the femoral nerve is not sending strong signals, the thigh muscle cannot do its job confidently.
Another real-world challenge is trust. After the knee buckles once, people often start walking differently to avoid another surprise. They may lock the knee, shorten their steps, lean to one side, or avoid stairs. These protective habits make sense, but over time they can create hip, back, or opposite-leg discomfort. Physical therapy helps not only by strengthening muscles but also by rebuilding trust in movement.
Sleep can also become annoying. Burning or tingling may feel worse at night because there are fewer distractions. Some people find that placing a pillow under the knees, avoiding positions that stretch the front of the hip too much, or changing sides more often can reduce irritation. However, new or worsening night pain should be discussed with a clinician, especially if it is severe or unexplained.
Recovery can test patience. Nerves heal slowly, and progress may arrive in tiny victories: one less stumble, one more stair, a stronger knee extension, a longer walk without fatigue. These wins matter. A person may not wake up one morning completely fixed, but they may realize they no longer need to grip the railing like it owes them money.
The emotional side deserves attention too. Leg weakness can make people feel older, less athletic, or suddenly cautious. That frustration is valid. It helps to track practical improvements rather than chasing perfection. Can you stand from a chair with less effort? Can you walk farther? Is numbness shrinking? Is the knee buckling less often? Those signs can show recovery even when symptoms have not disappeared.
Many people also learn that “exercise” does not mean crushing a workout. With femoral neuropathy, the right exercise is often humble: quad sets, controlled knee extensions, gentle hip mobility, and balance practice. These moves may not look impressive on social media, but they are exactly the kind of steady work that helps restore function. The goal is not to punish the leg into obedience. The goal is to coach the nerve-muscle team back into communication.
Finally, the best experience-based advice is simple: do not ignore weakness. Pain can be loud, but weakness is the clue that function is changing. If your thigh feels numb, your knee gives way, or stairs suddenly become a negotiation, get evaluated. Femoral neuropathy is manageable, but the smartest plan begins with knowing what is causing it.
Conclusion
Femoral neuropathy can affect comfort, confidence, and mobility because the femoral nerve plays a major role in thigh sensation, hip movement, and knee strength. Causes range from compression and trauma to surgery, diabetes-related nerve disease, bleeding, inflammation, or masses. Diagnosis often includes a physical exam, EMG and nerve conduction studies, blood tests, and imaging when needed.
Treatment works best when it targets the underlying cause while supporting recovery through pain control, physical therapy, safe strengthening, bracing if needed, and lifestyle changes. Exercises such as quad sets, heel slides, seated knee extensions, hip abduction, and balance training may help, but they should be tailored to the person’s symptoms and safety level.
The bottom line: thigh numbness plus knee weakness is not something to shrug off. With timely care and a thoughtful rehab plan, many people can improve function, reduce symptoms, and return to daily activities with more confidenceand fewer dramatic stairway negotiations.